

Introduction
Sleep quality is described as the feeling of a sleep experience, incorporating components of sleep initiation, maintenance, quantity, and enjoyment upon awakening (1). According to the American Academy of Sleep Medicine, an adult should sleep approximately seven or more hours per day (2). Poor sleep quality is closely linked to an increased susceptibility to a broad range of disorders, ranging from poor vigilance and memory to reduced mental and physical reaction times, reduced motivation, depression, insomnia, metabolic abnormalities, obesity, immune impairment, and even greater risk of cancer and cardiovascular disorders (3, 4). It is also linked to lower productivity and an increased chance of workplace injury (5, 6).
Worldwide, the prevalence of sleep problems ranges from 1.6% to 56.0% (7–9). Sleep problems are also common among healthcare professionals and significantly affect their quality of life, productivity, and ability to do their work (10). The prevalence of poor sleep quality among health professionals was 56.3% in Turkey (11), 73.8% in Vietnam (12), 86.8% in Malaysia (13), 42.3% in Saudi Arabia (14), 85.9% in Riyadh (10), and 54.2% in Nigeria (15). It is also estimated to be 53% in our country, Ethiopia (16). As a result, disturbed sleep or interrupted circadian rhythms may also initiate pathological condition in the human body (17). Additionally, factors including sex (18, 19), age (18, 20, 21), shift work (15, 22–24), coffee consumption (13), khat chewing (25, 26), alcohol consumption (20), depression (27, 28), not engaging in regular exercise (29–31), self-rated health (32), and extra use of smartphones are also among the most common risk factors of disturbed sleep–wake cycle (17).
Poor sleep quality can cause medical problems like fatigue and exhaustion, as well as psychological ones like increased irritation and loss of attention. These difficulties can impede communication and coordination among healthcare workers (29, 33, 34). Consequently, it is critical to investigate sleep quality and associated factors among healthcare workers (HCWs) in diverse settings in order to reduce the impact of sleep disorders and medical errors. Additionally, Ethiopian healthcare policy does not emphasize healthcare practitioners’ sleep quality (35). Despite the well-known link between sleep disturbances and a variety of severe health problems, research on sleep quality in Ethiopian healthcare professionals is limited (16, 36).
As a result, the current study is meant to fill this gap. Therefore, this study aimed to assess the prevalence of poor sleep quality and associated factors among healthcare professionals at the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia.
Materials and methods
Study setting
The study was conducted at the University of Gondar Comprehensive Specialized Hospital Northwest Ethiopia from February 1 to March 30, 2020. The University of Gondar Comprehensive Specialized Hospital is one of the biggest teaching hospitals in the Amhara region, serving over five million people requiring tertiary care. It is situated 728 km north of Ethiopia’s capital city, Addis Ababa. The hospital provides both comprehensive and referral-level treatment. There are 938 full-time registered healthcare workers. This research’s study population included all healthcare professionals working in the hospital.
Study design and population
An institution-based cross-sectional study was carried out among all healthcare workers who were permanently employed at the University of Gondar Comprehensive Specialized Hospital and were available during data collection. During the data collection time, healthcare professionals who were unable to communicate due to a serious illness were excluded.
Sample size determination and sampling procedure
The sample size for this study was determined using a single population proportion formula by assuming the prevalence of poor sleep quality among healthcare professionals (p = 50%), 95% confidence interval, and 5% margin of error. After adding a non-response rate of 10%, the final sample size became 423. There were a total of 876 healthcare professionals. Therefore, a stratified random sampling technique was applied based on their profession. First, a proportional allocation was used after identifying the number of healthcare workers in each profession. The study subjects were then chosen to form a total of 423 healthcare professionals using a computer-generated simple random sampling method from those strata.
Data collection tools and technique
Data were gathered from February 1 to March 30, 2020, using a self-administered questionnaire that included socio-demographic variables, work-related factors, substance use, depression (as assessed by the Beck’s Depression Inventory), and the Pittsburgh Sleep Quality Index (PSQI). The PSQI is a validated tool used to assess adult sleep quality and patterns (37). Subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, medication use, and daily dysfunction are the seven groups of the instrument. The seven domains are then added to create a total score, with a score greater than 5 indicating “poor” sleep quality and a score of less than or equal to 5 indicating “good” sleep quality (38).
Study variables
Poor sleep quality was the dependent variable in this research. Socio-demographic variables (age, gender, marital status, having children, and profession), substance use variables (alcohol consumption, cigarette smoking, drinking coffee, and khat chewing), work-related variables (working shift, working hour, and work experience), and health status variables (depression, history of chronic illness, exercise, and self-rated health) are independent variables. To assess depression, we used the Beck Depression Inventory (BDI), which is a 21-item self-report rating assessment that assesses depression-related attitudes and symptoms (39). The Beck Depression Inventory, second edition (BDI-II) is one of the most widely used tools in research and application to assess the existence and degree of depression in the previous 2 weeks (40). The BDI-II assesses 21 symptoms and attitudes, which include Mood, Pessimism, Sense of failure, Lack of satisfaction, Guilt feelings, Sense of punishment, Self-dislike, Self-accusation, Suicidal wishes, Crying, Irritability, Social withdrawal, Indecisiveness, Distortion of body image, Work inhibition, Sleep disturbance, Fatigability, Loss of appetite, Weight loss, Somatic preoccupation, and Loss of libido (41, 42). Participants with BDI-II scores ranging from 0 to 13 were deemed normal. Participants with BDI-II scores of 14–19, 20–28, or 29–63 were classified as having mild, moderate, or severe depression, respectively (39). In terms of substance use, participants were considered current substance users if they had used cigarettes, khat, alcohol, or coffee at least once in the month preceding the survey (43–45). Khat (Catha edulis) is an herbal trade-related cultivated plant growing in most parts of the world, particularly in Eastern Africa and Arab countries (46, 47). It contains psychoactive substances cathinone and cathine, which can cross the blood–brain barrier to enter and stimulate the brain (47–49). A semi-structured question “Did you have a previous history of chronic illness?” was used to evaluate the history of chronic illness. A “yes” answer was considered as having a history of chronic illness. The questionnaire assesses shift work by asking if they have day and night shift work; if they answer positively with “yes”, they were classified as having shift work. Shift work entails switching between day and night shifts. A healthcare shift worker is a healthcare professional who often works in a healthcare facility switching between day and night (50). Regular exercise is described as a subset of physical activity that is planned, structured, and repetitive, with the ultimate or intermediate goal of improving or maintaining physical health (51). According to WHO guidelines, 150–300 minutes of moderate-intensity physical exercise or 75–150 minutes of vigorous-intensity physical activity is recommended (52).
Statistical analysis
After checking for the completeness and consistency of the collected data, the data were entered into Epi-data version 3.02 and exported to SPSS version 25 for analysis. To express descriptive results, frequency with percent and mean with standard deviation were computed. The study fulfilled all chi-square assumptions, which assume that both factors are categorical, all observations are independent, and cells in the contingency table are mutually exclusive; there should be no zero cell values, and the expected value of cells should be 5 or higher in at least 80% of cells. A binary logistic regression was performed to determine the crude association between each independent variable and poor sleep quality. Variables in the bi-variable analysis with a p-value <0.25 were candidates for multivariable binary logistic regression analysis. The crude odds ratio (COR) and adjusted odds ratio (AOR) with 95% CI were calculated. For the multivariable analysis, variables with a p-value <0.05 were considered statistically significant.
Data quality management
To ensure the data quality, 1-day training was given for four BSc nursing data collectors. The questionnaire was also pretested, and regular supervision of the data collection process was also made to increase the completeness, accuracy, and consistency of the data. Incomplete questionnaires were discarded from the analysis. Cronbach’s alpha was also calculated to test the reliability of the PSQI tool, and it was 0.72.
Ethical consideration
Ethical clearance was obtained from the Ethical Review Board of the University of Gondar with ethical clearance number 1840/2012. To ensure the confidentiality of respondents, informed written consent was obtained from each study participant, and their names were not written on the questionnaire, which reduced the authors’ access to information that could identify individual participants during or after data collection.
Results
Socio-demographic characteristics of healthcare professionals
This survey had 418 participants. Initially, the plan was to collect data from 423 professionals, but due to incomplete and non-returned questionnaires, the response rate became 98.8%. Two hundred thirteen (51%) were female. The subjects’ mean age was 30.7 years (SD 6.3). One-third (33.3%) of the individuals were married. More than half of the participants in the research were nurses, 226 (54.1%), with midwives accounting for the remaining 60 (14.4%) (Table 1).
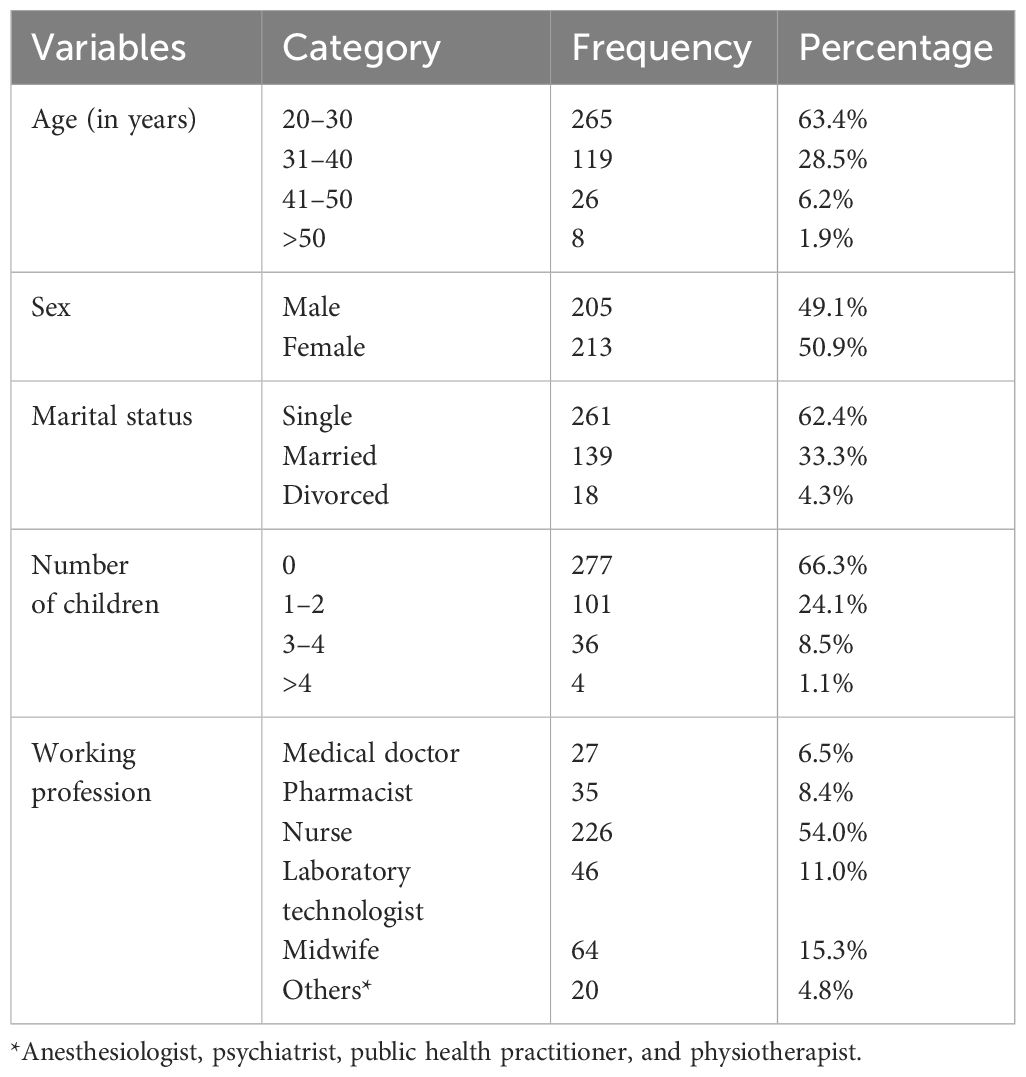
Table 1 Socio-demographic characteristics of healthcare professionals working at the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia, 2020 (n = 418).
Work- and health-related characteristics of the respondents
Three hundred eighty-five (92.1%) of the participants were on duty. Four hundred sixty (97.8%) of them worked fewer than 56 hours per week. In terms of substance use, 45 (10.8%), 260 (62.2%), and 35 (8.4%) of the subjects were current khat chewers, alcoholic drinkers, and cigarette smokers, respectively. Thirty-five (8.4%) of those who participated had a history of chronic disease. The majority of subjects (82.3%) reported moderate stress (Table 2).
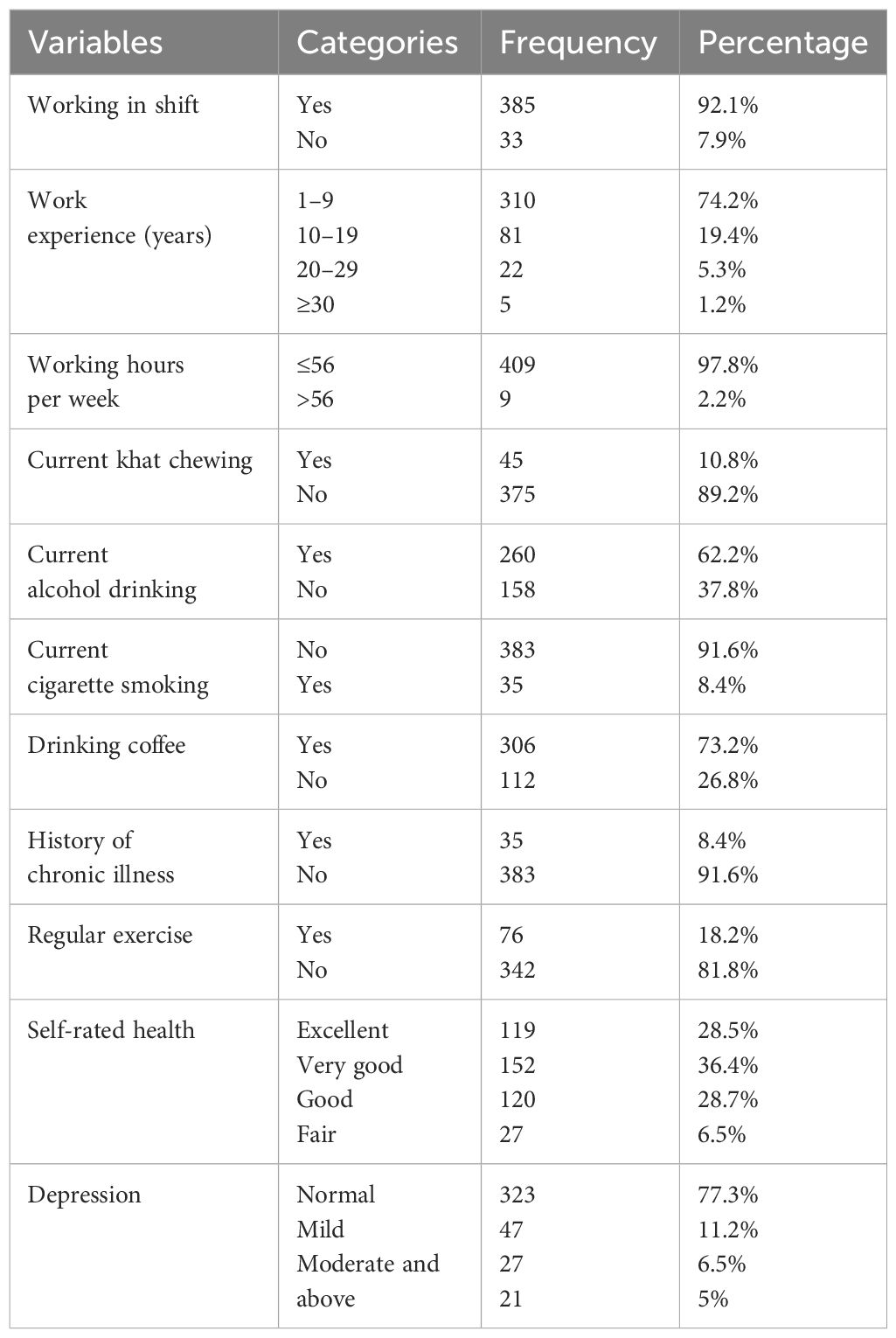
Table 2 Work- and health-related characteristics of healthcare professionals working at the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia, 2020 (n = 418).
Prevalence of poor sleep quality among healthcare professionals
The overall prevalence of poor sleep quality among healthcare professionals in this study was 58.9% [95% CI (54.2, 63.6%)]. Participants’ average night sleep duration and sleep latency were 6.5 hours (SD 1.27) and 18.6 minutes (SD 16.6), respectively. Three hundred five (73%) of the participants had less than 7 hours of sleep per day. Thirty-three (7.9%) and 73 (17.5%) had low habitual sleep efficiency (<65%) and used sleep medication in the past month, respectively (Table 3).
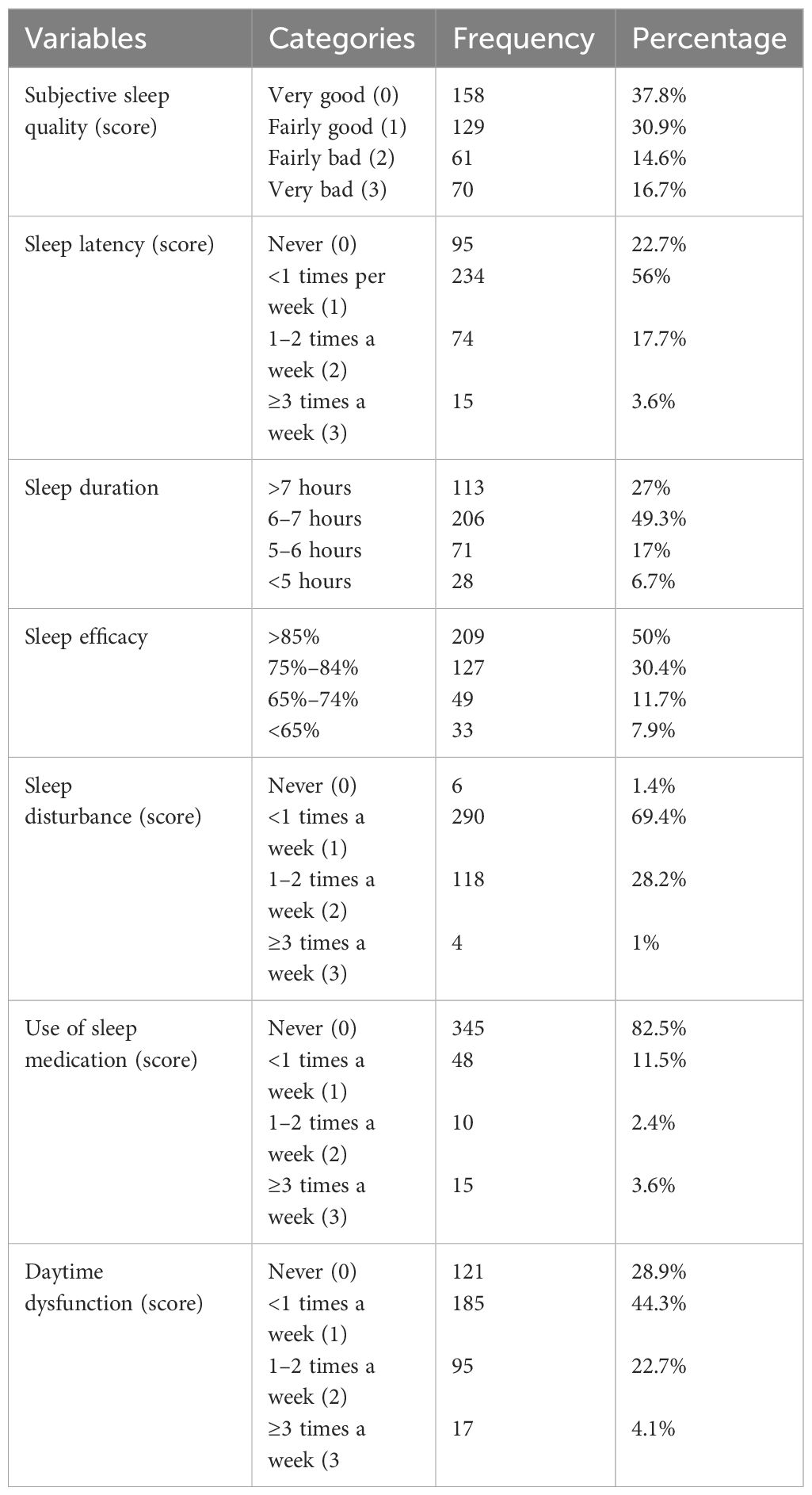
Table 3 Sleep quality and its component scores among healthcare professionals working at the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia, 2020 (n = 418).
Associated factors of poor sleep quality
In the logistic regression analysis, variables with p-value <0.25 were included in the multivariable logistic regression model. Accordingly, sex, shift work, current khat chewing, depression, and not performing exercise were significantly associated with poor sleep quality (p < 0.05).
Female participants were two times [AOR = 1.9, 95% CI (1.2, 2.9)] more likely to experience poor sleep quality compared to male participants. Participants who worked in shifts were six times [AOR = 5.7, 95% CI (2.3, 14.3)] more likely to have poor sleep quality than their counterparts. Participants who did not have regular exercise were two times more likely to have poor sleep quality than those who had regular exercise. Current khat chewers were three times [AOR = 3.1, 95% CI (1.2, 7.6)] more likely to experience poor sleep quality than those who did not chew khat. Participants with moderately severe depression were three times more likely to have poor sleep quality than those without depression [AOR = 2.6, 95% CI (1.3, 6.8)] (Table 4).
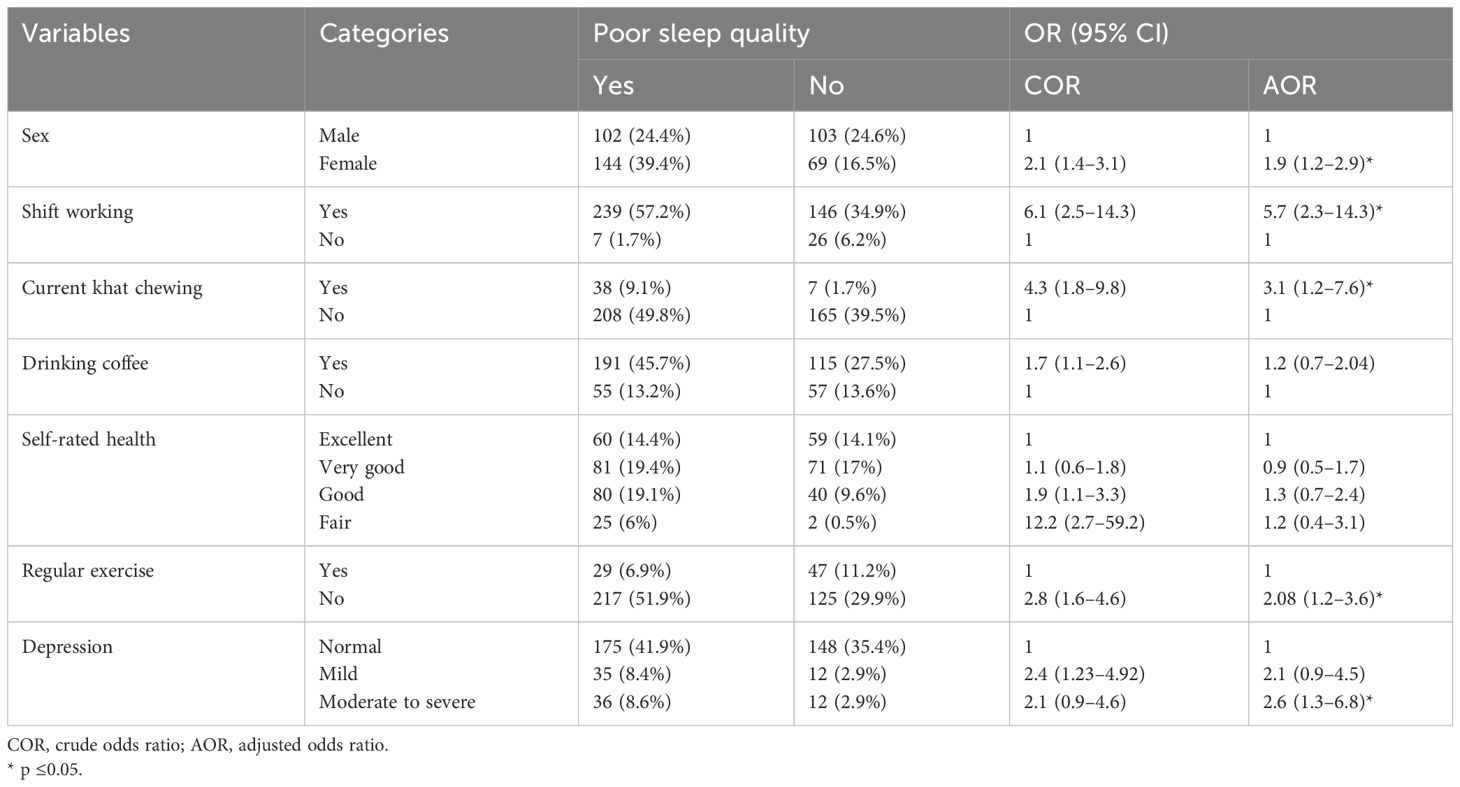
Table 4 Factors associated with poor sleep quality among healthcare professionals working at the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia, 2020 (n = 418).
Discussion
The current study aimed to determine the prevalence and risk factors for poor sleep quality among healthcare professionals at the University of Gondar Comprehensive Specialized Hospital. In this study, the prevalence of poor sleep quality was 58.9% [95% CI (54.2, 63.6%)], indicating that a significant number of participants are affected by the issue. This finding is in line with the results of studies conducted in Turkey (55.3%) (11), Malaysia (57.8%) (13), and Nigeria (54.2%) (15). Compared to previous studies in France (64.8%) (53), Mexico (56.7%) (28), Colombia (74.9%) (54), Saudi Arabia (73.4%) (55), Riyadh (85.9%) (10), China (75%) (56), Malaysia (86.8%) (13), and Ethiopia (70.6%) (57), this research discovered a lower prevalence of poor sleep quality among healthcare workers. Differences in study population could account for the disparity in prevalence of poor sleep quality among studies as a potential cause of this variation. Unlike the current study, which included participants from all healthcare professions, the previous studies only included nurses; this was the case in earlier Ethiopian and Chinese studies, as well as physicians in the Malaysian and Riyadh studies. Our study’s results outperform those of Nepal (48.03%) (58), Saudi Arabia (42.3%) (14), and Ethiopia (25.6%) (59). This disparity could be due to differences in the instrument used or differences in sample size. The previous research in Ethiopia, for example, used the shift work sleep disorder questionnaire to assess sleep quality, whereas the PSQI was used in this study.
The current research found sex, shift work, current khat chewing, depression, and a lack of regular exercise as determinants of poor sleep quality. Female gender was associated with an increased odds of poor sleep quality. A similar finding was reported from a study conducted in Austria (60), Pakistan (19), Spain (18), Saudi Arabia (61), and Ethiopia (62). This could be due to increased household and family responsibilities in women, which is typically associated with women working for extended periods of time at night, which could affect their sleep quality. Furthermore, in terms of the other differences in circadian timing between the sexes, it has been hypothesized that somewhat shorter circadian periods in women may cause them to be more out of circadian alignment, resulting in increased sleeplessness (63). This study also revealed that people who work in shifts have increased odds of poor sleep quality than non-shift workers. Consistent with the current study, studies in China (23), Spain (22), and Ethiopia (57) stated that people working in shifts had an increased risk of poor sleep quality than those working without shifts. A plausible explanation for this could be that working in a shift rotation could have an unpredictable working schedule that disrupts the circadian rhythm and restricts opportunities for sleep (15, 59).
As for the present study’s result, current khat chewers have demonstrated three times higher odds of poor sleep quality than non-khat chewers. This finding aligns with studies performed in Yemen and Ethiopia (25, 26, 62, 64). This could be due to the effect of khat. Because of its primary active ingredient (cathinone), khat (C. edulis) is initially a stimulant with effects similar to those of amphetamine (26, 65). However, this euphoric condition is typically followed by depression, irritability, anorexia, and sleeping difficulties. Cathinone’s effects are achieved by reduced dopamine uptake by nerve terminals, increased dopamine release, and inhibition of monoamine oxidase. As a result of the persistent stimulation of post-synaptic neurons following a high amount of dopamine in the synaptic cleft, all processes may result in poor sleep quality. After 8 hours of chewing, cathinone is scarcely detectable in the blood. The first-pass metabolism of cathinone in the liver results in the production of norepinephrine, which reduces sleep quality (20, 26, 66).
The present study found that participants who did not exercise regularly were more likely to have poor sleep quality, which is consistent with earlier research conducted in China and Brazil (29, 67, 68). This is because physical activity can produce positive changes in circadian rhythms and increase adenosine levels in the body, both of which help to regulate sleep (69). Furthermore, exercise promotes the production and release of melatonin, which frequently leads to improved sleep quality (70). This indicates that regular exercise, as recommended by WHO (71), is critical for reducing not only non-communicable diseases but also sleep problems, which is why the American Sleep Disorder Association recommends physical activity as a crucial non-medicinal intervention for sleep disorders (72).
The current research found a link between sleep quality and moderate-to-severe depressive symptoms. This result is congruent with research from Turkey, Saudi Arabia, China, and Ethiopia (27, 28, 73–75). This could be because people who suffer from depression have lower melatonin production and delays in the circadian rhythm of melatonin (76, 77). Another potential explanation is that in depressed people, nocturnal melatonin release is often reduced, which may be linked to sleep disturbances (78, 79).
Limitations of the study
Our study is not free from limitations. Because the study is cross-sectional, we are unable to show a cause–effect relationship between independent variables and poor sleep quality. Additionally, we could not show the dose–response relationship between substance use and sleep quality. Another limitation of this research could be recall bias.
Conclusion
The current study found that poor sleep quality was highly prevalent among healthcare providers at the University of Gondar Comprehensive Specialized Hospital and had significant associations with sex, shift work, khat chewing, exercise, and depressive symptoms. As a result, we recommend that healthcare providers at the University of Gondar’s Comprehensive and Specialized Hospital focus on early regular screening for sleep disturbances and pay special attention to shift work schedules and behaviors such as khat chewing, exercise, and depressive symptoms. Finally, we recommend other researchers perform additional investigations on factors like body mass index (BMI), sleep hygiene, and using the Internet, which have not been explored in the current research among healthcare professionals, because they have public health implications.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Ethical Review Board of University of Gondar. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
WT conceived the study, coordinated the process of data collection, was involved in data cleaning and statistical analysis, and prepared the first draft of the manuscript. AA, BD, AL, YA, and YY supervised the data collection process and participated in statistical analysis and interpretation of the results, manuscript reviewing, and editing. All authors contributed to the article and approved the submitted version.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The authors would like to express their genuine and heartfelt gratitude to the study participants and data collectors.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
2. Panel CC, Watson NF, Badr MS, Belenky G, Bliwise DL, Buxton OM, et al. Recommended amount of sleep for a healthy adult: a joint consensus statement of the American Academy of Sleep Medicine and Sleep Research Society. J Clin Sleep Med. (2015) 11:591–2. doi: 10.5664/jcsm.4758
PubMed Abstract | CrossRef Full Text | Google Scholar
3. Grandner MA, Jackson NJ, Pak VM, Gehrman PR. Sleep disturbance is associated with cardiovascular and metabolic disorders. J Sleep Res. (2012) 21:427–33. doi: 10.1111/j.1365-2869.2011.00990.x
PubMed Abstract | CrossRef Full Text | Google Scholar
4. Foster R. A good introduction to sleep and sleep disorders. Lancet Neurol. (2012) 11:848. doi: 10.1016/S1474-4422(12)70222-3
CrossRef Full Text | Google Scholar
5. Harvey AG, Stinson K, Whitaker KL, Moskovitz D, Virk H. The subjective meaning of sleep quality: a comparison of individuals with and without insomnia. Sleep. (2008) 31:383–93. doi: 10.1093/sleep/31.3.383
PubMed Abstract | CrossRef Full Text | Google Scholar
6. Nakata A, Ikeda T, Takahashi M, Haratani T, Fujioka Y, Fukui S, et al. Sleep-related risk of occupational injuries in Japanese small and medium-scale enterprises. Ind Health. (2005) 43:89–97. doi: 10.2486/indhealth.43.89
PubMed Abstract | CrossRef Full Text | Google Scholar
7. Koyanagi A, Stickley A. The association between sleep problems and psychotic symptoms in the general population: a global perspective. Sleep. (2015) 38:1875–85. doi: 10.5665/sleep.5232
PubMed Abstract | CrossRef Full Text | Google Scholar
8. Léger D, Poursain B, Neubauer D, Uchiyama M. An international survey of sleeping problems in the general population. Curr Med Res Opinion. (2008) 24:307–17. doi: 10.1185/030079907X253771
CrossRef Full Text | Google Scholar
9. Stranges S, Tigbe W, Gómez-Olivé FX, Thorogood M, Kandala N-B. Sleep problems: an emerging global epidemic? Findings from the INDEPTH WHO-SAGE study among more than 40,000 older adults from 8 countries across Africa and Asia. Sleep. (2012) 35:1173–81. doi: 10.5665/sleep.2012
PubMed Abstract | CrossRef Full Text | Google Scholar
10. Alamri FA, Amer SA, Almubarak A, Alanazi H. Sleep quality among healthcare providers; in Riyadh, 2019. Age (y). (2019) 20:30. doi: 10.18535/ijmsci/v6i5.03
CrossRef Full Text | Google Scholar
11. Esen AD, Mercan GN, Kaçar E, Toprak D. Sleep quality and related factors in medical residents. Turkish J Family Med Primary Care. (2017) 11:271–7. doi: 10.21763/tjfmpc.359842
CrossRef Full Text | Google Scholar
12. Phan T, Nguyen HPA, Dang CK, Phan MT, Nguyen VT, Tran BT, et al. Sleep Quality and Poor Sleep-related Factors among Healthcare Workers during the COVID-19 Pandemic in Vietnam. J Prev Med Public Health. (2023) 56:319. doi: 10.3961/jpmph.22.528
PubMed Abstract | CrossRef Full Text | Google Scholar
13. Ganasegeran K, Abdulrahman SA, Al-Dubai SAR, Rashid A, Perumal M, Renganathan P. Identifying factors associated with sleep disturbances among health workers using WhatsApp in Malaysia. J Hosp Manage Health Policy. (2017) 1:1–14. doi: 10.21037/jhmhp
CrossRef Full Text | Google Scholar
15. Kolo E, Ahmed A, Hamisu A, Ajiya A, Akhiwu B. Sleep health of healthcare workers in Kano, Nigeria. Nigerian J Clin Pract. (2017) 20:479–83. doi: 10.4103/1119-3077.204378
CrossRef Full Text | Google Scholar
16. Manzar MD, Bekele BB, Noohu MM, Salahuddin M, Albougami A, Spence DW, et al. Prevalence of poor sleep quality in the Ethiopian population: a systematic review and meta-analysis. Sleep Breathing. (2020) 24:709–16. doi: 10.1007/s11325-019-01871-x
PubMed Abstract | CrossRef Full Text | Google Scholar
17. Umar A, Khan MS, Sehgal SA, Jafar K, Ahmad S, Waheed A, et al. Epidemiological studies of sleep disorder in educational community of Pakistani population, its major risk factors and associated diseases. PloS One. (2022) 17:e0266739. doi: 10.1371/journal.pone.0266739
PubMed Abstract | CrossRef Full Text | Google Scholar
18. Madrid-Valero JJ, Martínez-Selva JM, Couto B, Sánchez-Romera JF, Ordoñana JR. Age and gender effects on the prevalence of poor sleep quality in the adult population. Gaceta sanitaria. (2017) 31:18–22. doi: 10.1016/j.gaceta.2016.05.013
PubMed Abstract | CrossRef Full Text | Google Scholar
19. Surani AA, Surani A, Zahid S, Ali S, Farhan R, Surani S. To assess sleep quality among Pakistani junior physicians (House officers): A cross−sectional study. Ann Med Health Sci Res. (2015) 5:329–33. doi: 10.4103/2141-9248.165246
PubMed Abstract | CrossRef Full Text | Google Scholar
20. Berhanu H, Mossie A, Tadesse S, Geleta D. Prevalence and associated factors of sleep quality among adults in Jimma Town, Southwest Ethiopia: a community-based cross-sectional study. Sleep Disord. (2018) 5:1–10. doi: 10.1155/2018/8342328
CrossRef Full Text | Google Scholar
21. Nazatul S, Saimy I, Moy FM, Nabila A. Prevalence of sleep disturbance among nurses in a Malaysian government hospital and its association with work characteristics. J Univ Malaya Med Centre (JUMMEC). (2008) 11:66–71. doi: 10.22452/jummec.vol11no2.5
CrossRef Full Text | Google Scholar
22. Gómez-García T, Ruzafa-Martínez M, Fuentelsaz-Gallego C, Madrid JA, Rol MA, Martínez-Madrid MJ, et al. Nurses’ sleep quality, work environment and quality of care in the Spanish National Health System: observational study among different shifts. BMJ Open. (2016) 6:e012073.22. doi: 10.1136/bmjopen-2016-012073
CrossRef Full Text | Google Scholar
23. Dai C, Qiu H, Huang Q, Hu P, Hong X, Tu J, et al. The effect of night shift on sleep quality and depressive symptoms among Chinese nurses. Neuropsychiatr Dis Treat. (2019) 15:435–40. doi: 10.2147/NDT
PubMed Abstract | CrossRef Full Text | Google Scholar
25. Ali AD, Al-Adhroey AH, Al-Shammakh AA, Mehrass AA-KO, Jaber HY, Mujlli HM. A pilot community-based study on association of Khat (Catha edulis) chewing practice with psychosis in Yemen. Am J Health Res. (2015) 3:91–6. doi: 10.11648/j.ajhr.20150302.16
CrossRef Full Text | Google Scholar
26. Jemere T, Mossie A, Berhanu H, Yeshaw Y. Poor sleep quality and its predictors among type 2 diabetes mellitus patients attending Jimma University Medical Center, Jimma, Ethiopia. BMC Res Notes. (2019) 12:1–6. doi: 10.1186/s13104-019-4531-6
PubMed Abstract | CrossRef Full Text | Google Scholar
27. Thichumpa W, Howteerakul N, Suwannapong N, Tantrakul V. Sleep quality and associated factors among the elderly living in rural Chiang Rai, northern Thailand. Epidemiol Health. (2018) 40. doi: 10.4178/epih.e2018018
PubMed Abstract | CrossRef Full Text | Google Scholar
28. Zurutuza JI, Ovando-Diego L, Lezama-Prieto MA, Morales-Romero J, Melgarejo-Gutierrez MA, Ortiz-Chacha CS, et al. Factors associated with poor sleep quality among primary healthcare workers during the SARS-CoV-2 pandemic. Cureus. (2024) 16(3). doi: 10.7759/cureus.56502
CrossRef Full Text | Google Scholar
29. Liu H, Liu J, Chen M, Tan X, Zheng T, Kang Z, et al. Sleep problems of healthcare workers in tertiary hospital and influencing factors identified through a multilevel analysis: a cross-sectional study in China. BMJ Open. (2019) 9:e032239. doi: 10.1136/bmjopen-2019-032239
PubMed Abstract | CrossRef Full Text | Google Scholar
30. Tan X, Saarinen A, Mikkola TM, Tenhunen J, Martinmäki S, Rahikainen A, et al. Effects of exercise and diet interventions on obesity-related sleep disorders in men: study protocol for a randomized controlled trial. Trials. (2013) 14:1–9. doi: 10.1186/1745-6215-14-235
PubMed Abstract | CrossRef Full Text | Google Scholar
31. Yang P-Y, Ho K-H, Chen H-C, Chien M-Y. Exercise training improves sleep quality in middle-aged and older adults with sleep problems: a systematic review. J Physiother. (2012) 58:157–63. doi: 10.1016/S1836-9553(12)70106-6
PubMed Abstract | CrossRef Full Text | Google Scholar
32. Ghalichi L, Pournik O, Ghaffari M, Vingard E. Sleep quality among health care workers. Arch Iranian Med. (2013) 16:0–.
Google Scholar
33. Alnofaiey YH, Alshehri HA, Alosaimi MM, Alswat SH, Alswat RH, Alhulayfi RM, et al. Sleep disturbances among physicians during COVID-19 pandemic. BMC Res Notes. (2020) 13:1–7. doi: 10.1186/s13104-020-05341-6
PubMed Abstract | CrossRef Full Text | Google Scholar
35. Durmer JS, Dinges DF eds. Neurocognitive consequences of sleep deprivation. Seminars in neurology. 333 Seventh Avenue, New: Copyright© 2005 by Thieme Medical Publishers, Inc. (2005).
Google Scholar
37. Salahuddin M, Maru TT, Kumalo A, Pandi-Perumal SR, Bahammam AS, Manzar MD. Validation of the Pittsburgh sleep quality index in community dwelling Ethiopian adults. Health Qual Life Outcomes. (2017) 15:1–7. doi: 10.1186/s12955-017-0637-5
PubMed Abstract | CrossRef Full Text | Google Scholar
38. Buysse DJ, Reynolds CF III, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. (1989) 28:193–213. doi: 10.1016/0165-1781(89)90047-4
PubMed Abstract | CrossRef Full Text | Google Scholar
39. Gebrie MH. An analysis of beck depression inventory 2nd edition (BDI-II). USA: Global Journal of Endocrinological metabolism. (2020). 2(3). doi: 10.31031/GJEM.2018.02.000540
CrossRef Full Text | Google Scholar
40. Joe S, Woolley ME, Brown GK, Ghahramanlou-Holloway M, Beck AT. Psychometric properties of the Beck Depression Inventory–II in low-income, African American suicide attempters. J Pers Assess. (2008) 90:521–3. doi: 10.1080/00223890802248919
PubMed Abstract | CrossRef Full Text | Google Scholar
41. Canel-Çınarbaş D, Cui Y, Lauridsen E. Cross-cultural validation of the Beck depression inventory–II across US and Turkish samples. Measurement Eval Couns Dev. (2011) 44:77–91. doi: 10.1177/0748175611400289
CrossRef Full Text | Google Scholar
42. Al-Turkait FA, Ohaeri JU. Dimensional and hierarchical models of depression using the Beck Depression Inventory-II in an Arab college student sample. BMC Psychiatry. (2010) 10:1–14. doi: 10.1186/1471-244X-10-60
PubMed Abstract | CrossRef Full Text | Google Scholar
43. Eticha T, Kidane F. The prevalence of and factors associated with current smoking among College of Health Sciences students, Mekelle University in northern Ethiopia. PloS One. (2014) 9:e111033. doi: 10.1371/journal.pone.0111033
PubMed Abstract | CrossRef Full Text | Google Scholar
44. Yeshaw Y, Zerihun MF. Khat chewing prevalence and correlates among university staff in Ethiopia: a cross-sectional study. BMC Res Notes. (2019) 12:1–6. doi: 10.1186/s13104-019-4706-1
PubMed Abstract | CrossRef Full Text | Google Scholar
45. Getachew T, Defar A, Teklie H, Gonfa G, Bekele A, Bekele A, et al. Magnitude and predictors of excessive alcohol use in Ethiopia: Findings from the 2015 national non-communicable diseases STEPS survey. Ethiopian J Health Dev. (2017) 31:312–9.
Google Scholar
46. Corkery JM, Schifano F, Oyefeso A, Ghodse AH, Tonia T, Naidoo V, et al. Overview of literature and information on” khat-related” mortality: a call for recognition of the issue and further research. Annali dell’Istituto superiore di sanità. (2011) 47:445–64. doi: 10.4415/ANN_11_04_17
PubMed Abstract | CrossRef Full Text | Google Scholar
47. Gashawa A, Getachew T. The chemistry of khat and adverse effect of khat chewing. Am Sci Res J Eng Technol Sci. (2014) 9:35–46.
Google Scholar
48. Al-Motarreb A, Al-Habori M, Broadley KJ. Khat chewing, cardiovascular diseases and other internal medical problems: the current situation and directions for future research. J Ethnopharmacol. (2010) 132:540–8. doi: 10.1016/j.jep.2010.07.001
PubMed Abstract | CrossRef Full Text | Google Scholar
49. Organization WH. WHO Expert Committee on Drug Dependence: thirty-fourth report. Geneva: World Health Organization (2006).
Google Scholar
50. Dires T, Feleke DG, Amera T, Bante B, Tsedalu A, Birhanu A, et al. Assessment of night-shift effects on nurses’ health and work performance at South Gondar zone public hospitals, 2022. Int J Afr Nurs Sci. (2023) 18:100530. doi: 10.1016/j.ijans.2023.100530
CrossRef Full Text | Google Scholar
51. Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. (1985) 100:126.
PubMed Abstract | Google Scholar
52. Bull FC, Al-Ansari SS, Biddle S, Borodulin K, Buman MP, Cardon G, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. (2020) 54:1451–62. doi: 10.1136/bjsports-2020-102955
PubMed Abstract | CrossRef Full Text | Google Scholar
53. Coelho J, Lucas G, Micoulaud-Franchi J-A, Philip P, Boyer L, Fond G. Poor sleep is associated with work environment among 10,087 French healthcare workers: Results from a nationwide survey. Psychiatry Res. (2023) 328:115448. doi: 10.1016/j.psychres.2023.115448
PubMed Abstract | CrossRef Full Text | Google Scholar
54. Waich A, Barahona-Correa JE, del Carmen Figueredo M, Rondón-Sepúlveda MA, Ruiz AJ, Castellanos JC, et al. Sleep Quality, Insomnia, and Perceived Stress among Colombian Healthcare Workers during the COVID-19 Pandemic. Sleep Sci. (2023) 16:044–50. doi: 10.1055/s-0043-1767756
CrossRef Full Text | Google Scholar
55. Alameri RA, Almulla HA, Al Swyan AH, Hammad SS. Sleep quality and fatigue among nurses working in high-acuity clinical settings in Saudi Arabia: a cross-sectional study. BMC Nurs. (2024) 23:51. doi: 10.1186/s12912-023-01693-z
PubMed Abstract | CrossRef Full Text | Google Scholar
57. Olana DD, Ayana AM, Abebe ST. Sleep quality and its associated factors among nurses in jimma zone public hospitals, Southwest Ethiopia, 2018. Sleep Hypnosis (Online). (2019) 21:271–80. doi: 10.37133/Sleep.Hypn.2019.21.0197
CrossRef Full Text | Google Scholar
58. Kafle B, Tiwari S, Pokhrel A, Shrestha R, Bagale Y, Pahari N. Poor quality of sleep among healthcare workers in a tertiary care centre. JNMA: J Nepal Med Assoc. (2024) 62:118. doi: 10.31729/jnma.8435
PubMed Abstract | CrossRef Full Text | Google Scholar
59. Haile KK, Asnakew S, Waja T, Kerbih HB. Shift work sleep disorders and associated factors among nurses at federal government hospitals in Ethiopia: a cross-sectional study. BMJ Open. (2019) 9:e029802. doi: 10.1136/bmjopen-2019-029802
PubMed Abstract | CrossRef Full Text | Google Scholar
60. Tmava-Berisha A, Fellendorf FT, Ratzenhofer M, Maget A, Platzer M, Bengesser SA, et al. Sleep quality among workers in the health sector exposed to the COVID-19 pandemic. PloS One. (2022) 17:e0268933. doi: 10.1371/journal.pone.0268933
PubMed Abstract | CrossRef Full Text | Google Scholar
61. Darraj A, Mahfouz MS, Alsabaani A, Sani M, Alameer A. Assessment of sleep quality and its predictors among patients with diabetes in Jazan, Saudi Arabia. Diabetes Metab Syndr Obes: Targets Ther. (2018) 11:523–31. doi: 10.2147/DMSO
CrossRef Full Text | Google Scholar
62. Abate H, Letta S, Worku T, Tesfaye D, Amare E, Mechal A. Shiftwork sleep disorder and associated factors among nurses working at public hospitals in Harari Regional state and Dire Dawa Administration, Eastern Ethiopia: a cross-sectional study. BMC Nurs. (2023) 22:118. doi: 10.1186/s12912-023-01257-1
PubMed Abstract | CrossRef Full Text | Google Scholar
63. Gentry N, Ptacek L, Fu Y-H. Genetic and biological factors in sleep. Foundations Sleep Health: Elsevier;. (2022) p:73–95. doi: 10.1016/B978-0-12-815501-1.00001-6
CrossRef Full Text | Google Scholar
64. Manzar MD, Salahuddin M, Alamri M, Maru TT, Pandi-Perumal SR, Bahammam AS. Poor sleep in concurrent users of alcohol, khat, and tobacco smoking in community-dwelling Ethiopian adults. Ann Thorac Med. (2018) 13:220. doi: 10.4103/atm.ATM_36_18
PubMed Abstract | CrossRef Full Text | Google Scholar
66. Abebe M, Kindie S, Adane K. Adverse health effects of khat: a review. Fam Med Med Sci Res. (2015) 4(1):2–5. doi: 10.4172/2327-4972.1000154
CrossRef Full Text | Google Scholar
67. Carvalho VP, Barcelos KA, Oliveira E, Marins SN, Rocha IBS, Sousa D, et al. Poor sleep quality and daytime sleepiness in health professionals: prevalence and associated factors. Int J Environ Res Public Health. (2021) 18:6864. doi: 10.3390/ijerph18136864
PubMed Abstract | CrossRef Full Text | Google Scholar
68. Tian Y, Yue Y, Yang J, Chen H, Lu L, Zhou J, et al. Sociodemographic, occupational, and personal factors associated with sleep quality among Chinese medical staff: A web-based cross-sectional study. Front Public Health. (2022) 10:1060345. doi: 10.3389/fpubh.2022.1060345
PubMed Abstract | CrossRef Full Text | Google Scholar
69. Karimi S, Soroush A, Towhidi F, Makhsosi BR, Karimi M, Jamehshorani S, et al. Surveying the effects of an exercise program on the sleep quality of elderly males. Clin Interventions Aging. (2016) 11(1):997–1002. doi: 10.2147/CIA.S106808
CrossRef Full Text | Google Scholar
71. Engelsman EL. The World Health Organization Global Recommendations on Physical Activity for Health and the Opportunities for the Sports World. Promoting Sport for All Benefits and Strategies for the 21st Century, Vol. 93. Geneva: WHO. (2010).
Google Scholar
72. Baron KG, Reid KJ, Malkani RG, Kang J, Zee PC. Sleep variability among older adults with insomnia: associations with sleep quality and cardiometabolic disease risk. Behav Sleep Med. (2017) 15:144–57. doi: 10.1080/15402002.2015.1120200
PubMed Abstract | CrossRef Full Text | Google Scholar
73. Dağ B, Kutlu FY. The relationship between sleep quality and depressive symptoms in adolescents. Turkish J Med Sci. (2017) 47:721–7. doi: 10.3906/sag-1507-14
CrossRef Full Text | Google Scholar
74. Guo L, Deng J, He Y, Deng X, Huang J, Huang G, et al. Prevalence and correlates of sleep disturbance and depressive symptoms among Chinese adolescents: a cross-sectional survey study. BMJ Open. (2014) 4:e005517. doi: 10.1136/bmjopen-2014-005517
PubMed Abstract | CrossRef Full Text | Google Scholar
75. Lemma S, Gelaye B, Berhane Y, Worku A, Williams MA. Sleep quality and its psychological correlates among university students in Ethiopia: a cross-sectional study. BMC Psychiatry. (2012) 12:1–7. doi: 10.1186/1471-244X-12-237
PubMed Abstract | CrossRef Full Text | Google Scholar
76. Claustrat B, Chazot G, Brun J, Jordan D, Sassolas G. A chronobiological study of melatonin and cortisol secretion in depressed subjects: plasma melatonin, a biochemical marker in major depression. Biol Psychiatry. (1984) 19:1215–28. doi: 10.1046/j.1468-2982.1984.0404213.x
PubMed Abstract | CrossRef Full Text | Google Scholar
78. Salgado-Delgado R, Tapia Osorio A, Saderi N, Escobar C. Disruption of circadian rhythms: a crucial factor in the etiology of depression. Depression Res Treat. (2011) 2011. doi: 10.1155/2011/839743
CrossRef Full Text | Google Scholar
79. Et D, de L’Humeur TDT. Resetting the internal clock in depression: AN ew therapeutic approach. Medicographia. (2007) 29(1). doi: 10.1097/01.yic.0000277957.75852.c7
CrossRef Full Text | Google Scholar
link